Tag: one health
-

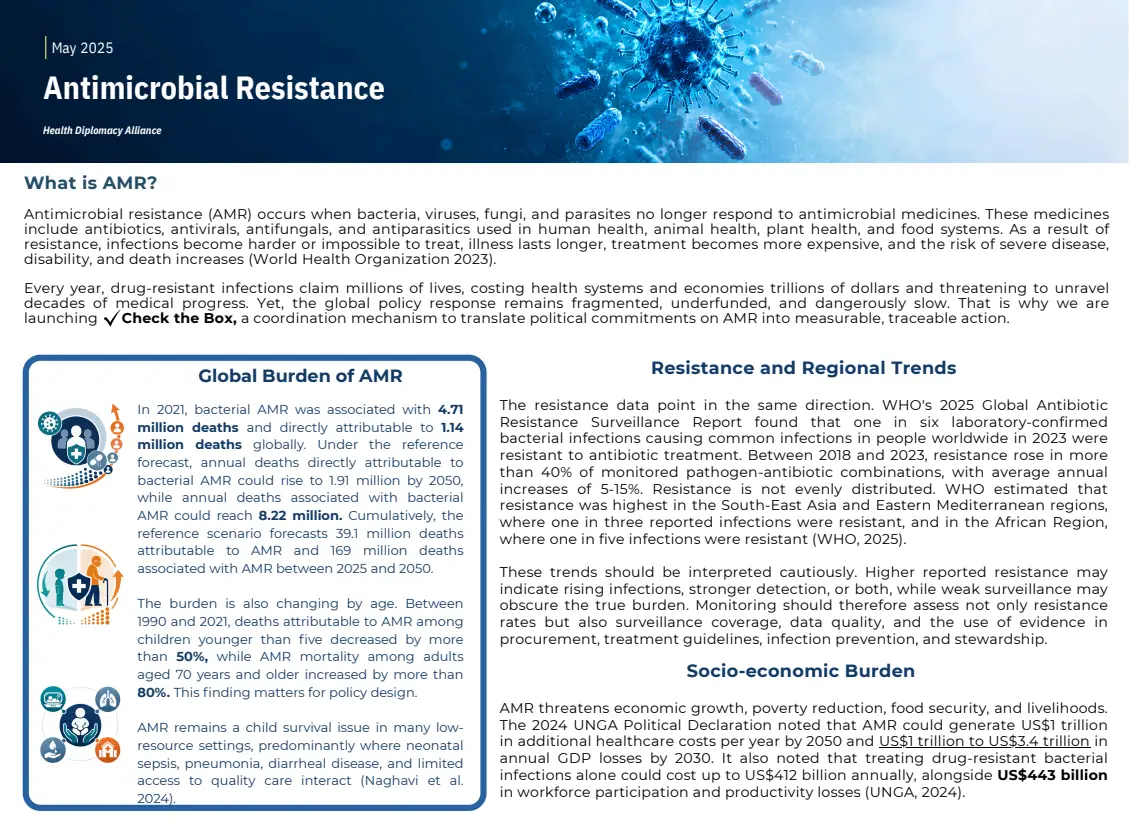
WHO Launches Civil Society Task Force on AMR
In a significant step to strengthen global action against antimicrobial resistance (AMR), the World Health Organization (WHO) launched the Civil Society Task Force on AMR during World Antimicrobial Awareness Week (WAAW) 2025. The initiative brings together nongovernmental organizations and civil society groups from around the world to coordinate efforts, provide evidence, identify gaps, and promote engagement between governments, communities, and stakeholders.
The Task Force aims to amplify the voices of affected communities and ensure that civil society organizations can contribute meaningfully to global strategies to combat AMR. Its objectives include fostering collaboration across sectors, supporting capacity building, promoting advocacy, and advancing WHO’s GPW14.
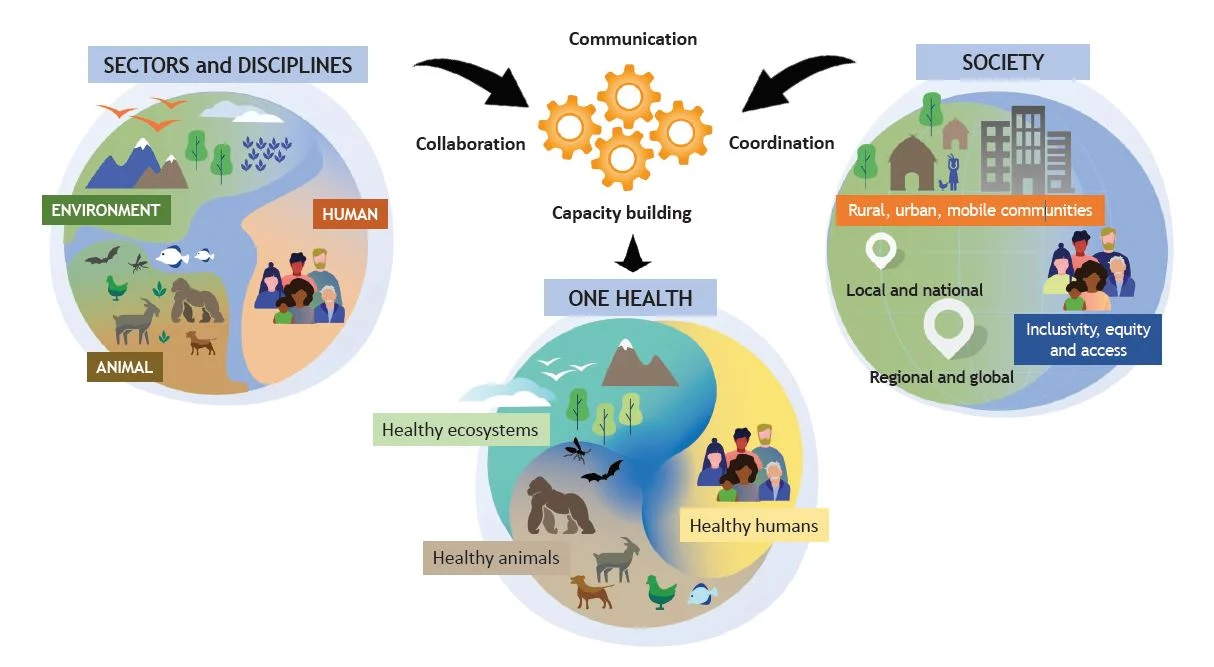
The Health Diplomacy Alliance (HDA) will be co-sharing the Steering Committee of the Task Force, bringing expertise in health diplomacy and cooperation. HDA’s involvement strengthens efforts to highlight the impact of AMR at global, regional, and national levels, while supporting civil society to engage in advocacy, strengthen regulatory systems, increase access to quality-assured antimicrobials, and integrate the One Health Approach into planning.
AMR continues to pose a severe global health threat. In 2019, drug-resistant infections were associated with approximately 4.95 million deaths, and by 2021, an estimated 1.14 million deaths were directly attributable to AMR. Without effective measures, healthcare costs could rise by $1 trillion by 2050.
By including civil society voices alongside technical expertise, the Task Force ensures that AMR responses are locally grounded, equitable, and evidence-based, helping governments and communities implement effective, sustainable solutions.
HDA’s participation in the Task Force underscores its commitment to promoting long-term, political system-level solutions to address the growing challenge of antimicrobial resistance.
-

Invisible Emergencies: Climate Change, Mental Health, and Health Diplomacy
As climate impacts intensify, exacerbating trauma, food insecurity, displacement, and health inequities, mental health continues to be overlooked in climate strategies, underscoring the need for integrated action. Held in the wake of the Health Day deliberations at COP30, the webinar organized by the Health Diplomacy Youth Network responded to growing recognition of the psychological toll of climate change on vulnerable and climate-affected communities. With participation from youth leaders, environmental psychology experts, and community mental health practitioners, the session brought mental health to the forefront of climate diplomacy.
Ayesha Ali, Coordinator of the Commonwealth Youth Health Network, opened the session by highlighting the gap between policy commitments and real-world access to mental health services in climate-vulnerable regions, especially for women, rural populations, and young people.
Matteo Consiglio, Lead, Food and Water Systems, Swiss Youth for Climate, underscored how climate-driven food insecurity contributes to anxiety, stress, and psychosocial instability, calling for stronger links between food systems, environment, and public health.
Dr. Jakub S. Bil, Universal Health Coverage Working Group Co-Chair, Global Mental Health Action Network, emphasized community-based and rights-based mental health approaches, noting that climate impacts frequently compound pre-existing trauma and inequities, and stressed co-design of solutions with affected communities as central to sustainable implementation.
Dr. Harshita Umesh, Focal Point, Health Working Group, YOUNGO, highlighted the limited integration of mental health within UNFCCC processes and called for mental health to be embedded across adaptation and disaster response mechanisms, while Dion Ras, Executive Committee Member, International Association for Youth Mental Health, brought a grassroots lens, emphasizing peer support, lived experience, and the need for accessible, youth-informed systems of care in the face of climate stressors.
During the panel discussion, Ebunoluwa Ayinmode steered a conversation that underscored the gap between policy ambition and implementation, the invisibility of cumulative climate-related trauma in formal frameworks, and the need for health diplomacy to align institutions, communities, and youth constituencies around shared priorities
This event marks an important step in elevating the climate–mental health objectives enshrined in the Belem Health Action Plan by mobilizing diverse expertise, amplifying youth and community voices, and identifying practical pathways for integrated, equity-focused action. The Health Diplomacy Youth Network remains committed to advancing diplomatic engagement, intergenerational collaboration, and evidence-based advocacy to ensure that mental health becomes a central pillar of climate resilience.